Bimonthly Internal assessment for December
"This is my submission for the Bimonthly internal assessment for the month of December."
Most of the information here have been collected from different reference sites, links to which have been mentioned.The points copy pasted have been put in quotes.
The questions to the cases being discussed are from the link below:
https://medicinedepartment.blogspot.com/2020/12/medicine-question-paper-for-december.html?m=1
1) A 55 year old man with Recurrent Focal Seizures
Detailed patient case report here: http:/ushaindurthi.
1. What is the problem representation of this patient and what could be the anatomical site of lesion ?
Ans) This is a case of 55 year old with complaint that he is unable to move his right upper limb followed by sudden onset of tonic clonic seizure involving right upper limb and right lower limb for about 2 minutes followed by another 8 episodes of tonic clonic seizures involving the right upper limb and lower limb, the episodes lasted for 2 minutes and there was a gap between each episode which was about 2 minutes.
He is a known case of type 2 diabetes on metformin since 5 years
Anatomical site of lesion: acute ischemic infarct of the left fronto parietal region,this is the cause of the hemiplegia and also the cause of seizures continuously.
2. Why are subcortical internal capsular infarcts more common that cortical infarcts?
Ans)The cortex is supplied by the short and long cortical branches of cerebral artery and deep portion of white matter is supplied by central branches of cerebral artery leaving a zone of diminished nutrition at the subcortical internal capsular region, this shows that subcortical infarcts are more common than cortical Infarcts.
Reference: text book of clinical neuro anatomy by vishraam singh 2nd edition page no:179
3. What is the pathogenesis involved in cerebral infarct related seizures?

4. What is your take on the ecg? And do you agree with the treating team on starting the patient on Enoxaparin?
If so why?
Ventricular ectopics,
poor R Wave progression,
left axis deviation is seen in the ECGs of the patient
NSTEMI in anteroseptal leads.
Enoxoparin given post stroke to prevent the emboli from travelling to the heart or lungs and causing cardiac arrest or pulmonary embolism, it is superior to LMWH or unfractioned heparin in preventing venous thromboembolism in patients with acute ischemic stroke
Source: http:/ushaindurthi.
5. Which AED would you prefer?
Monotherapy is sufficient in late post stroke seizures patients. Leviteracetam and lamotrigine can be used in post stroke seizures to maintain longterm seizure free period,as they have fewer interactions with other drugs especially enoxoparin(anticoagulant being used in this patient).
Source: https://www.slideshare.net/mobile/DrSudhirKumar4/post-stroke-epilepsy
Please provide studies on efficacies of each of the treatment given to this patient.
Levipil : for seizures
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2526377/
Questions:
1. What is the problem representation for this patient?
Answer) patient has complaints of SOB varies between Grade 2-3 which increased on exertion since 3 days with complaints of cough not associated with sputum production2. What is the cause for his recurrent hypoglycemia? And how would you evaluate?
This patient is on glimi- M1 as mentioned in the history - antidiabetic drug that raises insulin levels independently( even though the blood glucose levels are low) and also this patient is on mixtard insulin which is the cause of his reccurent hypoglycemia, a combination of these both drugs or sulfonylureas) in relation to food intake and physical activity levels.
Decreased endogenous glucose production (eg, after alcohol intake)
3. What is the cause for his Dyspnea? What is the reason for his albumin loss?
Patient has pneumonia which is the reason for his dyspnea and also he has repeated episodes of hypoglycaemia due to sepsis which is also one of the cause for his breathlessness.
The main causes of proteinuria in this case is high blood glucose levels over a period of years(diabetic nephropathy). High blood pressure might also have lead to the development of kidney damage
source: https://www.diabetes.co.uk/diabetes-complications/proteinuria.html
4. What is the pathogenesis involved in hypoglycemia ?

https://pubmed.ncbi.nlm.nih.gov/29061311/
https://trialbulletin.com/lib/trials/term=Insulin+NovoRapid+versus+Actrapid
3)
A. 41 year old man with Polyarthralgia
Case details here: https://
1. How would you evaluate further this patient with Polyarthralgia?
To rule out gout-RFT should be done as the value of uric acid is 5.3, it is ruled out
To rule out infectious causes( as the patient has intermittent fever with chills and rigors)
To rule out hodgkins lymphoma( as patient has fever with chills and rigors,weight loss, and joint pains but not bone pains) but the patient has no lymph node swellings
Patient has early morning stiffness and joint space tenderness,fever,small joints of hand and foot, ankle and wrist ,large joints of knee, shoulders are involved and on clinical examination there was ulnar deviation of fingers and radial deviation of metacarpal bones and piano key deformity suggestive of RHEUMATOID ARTHRITIS
CBP shows anemia(normocytic and normochromic) and lymphocytopenia
2. What is the pathogenesis involved in RA?

Pathogenesis:” Rheumatoid arthritis (RA) is an autoimmune systemic disease that primarily affects joints. Etiology and the pathogenesis of RA are complex, involving many types of cells, among others macrophages, T and B cells, fibro- blasts, chondrocytes and dendritic cells. Despite well documented role of many genes and epigenetic modifications in the development and evolution of the disease, in most RA patients there is no clear predisposing factor present. Environmental factors involved in RA pathogenesis are cigarette smoke, industrial pollutants like silica crystals, disturbances of intestinal, lung, and oral microbiota and some specific bacterial and viral infectious agents and their components. In the initial disease stage there are qualitative and quantitative disturbances ofpeptide citrulination as well as other protein modifications, followed by antigen presenting cell (APC) (macrophages and dendritic cells) and fibroblast like synoviocytes (FLS) activation. Some microbes foster this processes by APC and FLS direct and indirect activation. In the second stage APC's elicit specific humoral B cell re- sponse resulting in specific antibodies production and T cell autoreactivity. Inherited and acquired defects in T and B cell responses caused by repeated activation of innate immunity as well as loss of tolerance, elicit chronic autoimmune inflammation, primarily of synovial membranes, and development of cellular panus. Pathologic activation of the osteoclasts and release of the immune system effector molecules and the proteolytic enzymes damage the cartilage, bone and tendons composition and structure. Persistent inflammation through its complex mechanisms results in many systemic and extraarticular RA manifestations of almost all organ systems, resulting in severe complications and comorbidities such as rheumatoid lung, carditis, vasculitis, cahexia, anemia, accelerated atherosclerosis, myocardial and cerebrovascular vascular disease, lymphoma, osteoporosis, depression etc. Accumulated complications and comorbidities finally result in handicap, social dysfunction and premature death.
Source: https://pubmed.ncbi.nlm.nih.gov/25427390/
3. What are the treatment regimens for a patient with RA and their efficacies?

https://ard.bmj.com/content/79/6/744
B.
75 year old woman with post operative hepatitis following blood transfusion
Case details here: https://
1.What are your differentials for this patient and how would you evaluate?
Post operative hepatic failure
Post transfusion hepatitis
Ischemic hepatitis
Evaluation is done by ABO AND RH compatibility, coombs test. In LFT there would be rise in bilirubin levels both total and and direct bilirubin, elevated alkaline phosphatase and total proteins and albumin would decrease due to rapid deterioration in liver function and hematuria( causing a decrease in levels of hemoglobin along with a dramatic raise in LDH levels, ESR is higly elevated as seen in this case and patient clinically shows jaundice with fever,chills and rigors and coombs test also should be done.
2. What would be your treatment approach? Do you agree with the treatment provided by the treating team and why? What are their efficacies?
Yes I agreee with the treatment Being done to this patient.
Symptomatic treatment should be given in this case
To prevent hepatic encephalopathy lactulose is being given.
Efficacy: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0104-42302016000300243
To prevent any gastritis pantop is being given
Efficacy: https://www.researchgate.net/publication/5466323_Proton_pump_inhibitors_and_gastritis
To prevent vomitings zofer is being given
Efficacy: https://clinicaltrials.gov/ct2/show/NCT02028910
For wheezing and crepts: nebulisation is being done with mucomist,budecort and duolin.
UDILIV is used for primary biliary cirrhosis
4) 60 year woman with Uncontrolled sugars
http://manojkumar1008.
1. What is the problem representation of this patient?
60 year female with chest pain since 4 days pricking type,radiating to back which got releived when patient took pain killers,patient is a known case of diabetes and hypertension since 2 years on medication but not controlled secondary to right upper lobe consolidation with sepsis.
She was diagnosed with AKI with septic shock with dyselectrolytemia 1.5 years back
2. What are the factors contributing to her uncontrolled blood sugars?
The patient has underlying sepsis which is the leading cause of her uncontrolled blood sugars in the last few days. The foci of sepsis is the right upper lobe consolidation as seen in X ray
3. What are the chest xray findings?
Answer) Right upper lobe consolidation might be indicative of Pneumonia.
Trachea is shifted towards right
Heart is central in position, size is normal
4. What do you think is the cause for her hypoalbuminaemia? How would you approach it?
Inflammation In this case uncontrolled diabetes leads to diabetic nephropathy,in which there is loss of albumin in the urine ultimately causing hypoalbuminaemia.

Source:
https://www.semanticscholar.org/paper/Albumin-in-Health-and-Disease%3A-Causes-and-Treatment-Throop-Kerl/993f1361d9992d3102233c70730236b2258360c4
5. Comment on the treatment given along with each of their efficacies with supportive evidence.
Patient was given antibiotics for the pneumonia
Egg white and protein powders for hypoalbuminameia
Zofer for vomitings
Efficacy: https://clinicaltrials.gov/ct2/show/NCT02028910
Lactulose for constipation
Efficacy: https://pubmed.ncbi.nlm.nih.gov/21510584/
Tramadol for pain
Efficacy: https://www.sciencedirect.com/science/article/pii/S0753332218373694
Actrapid for sugar control
Efficacy: https://pubmed.ncbi.nlm.nih.gov/6343041/
Pantop is given for gastritis
Efficacy: https://www.researchgate.net/publication/5466323_Proton_pump_inhibitors_and_gastritis
5) 56 year old man with Decompensated liver disease
Case report here: https://appalaaishwaryareddy.
1. What is the anatomical and pathological localization of the problem?
The patient has cirrhosis secondary to HBV infection
Source: https://www.emjreviews.com/hepatology/article/immunopathogenesis-of-hepatitis-b-virus-infection-and-related-complications/
~AKI on ckd ( hepatorenal syndrome)
~Pneumonia and pleural effusion
2. How do you approach and evaluate this patient with Hepatitis B?
As this is a known case of hepatitis B and patient has developed complications such as ascites,pleural effusion and jaundice the following measures to be taken.
Liver function tests to assess the level of liver damage which shows elevated levels of direct and total bilirubin indicating liver cirrhosis in this patient also ascites is seen in clinical examination and also pitting type of edema indicating low protein levels- protein powder should be given and protein intake should be increased
The patient also shows deranged RFTs
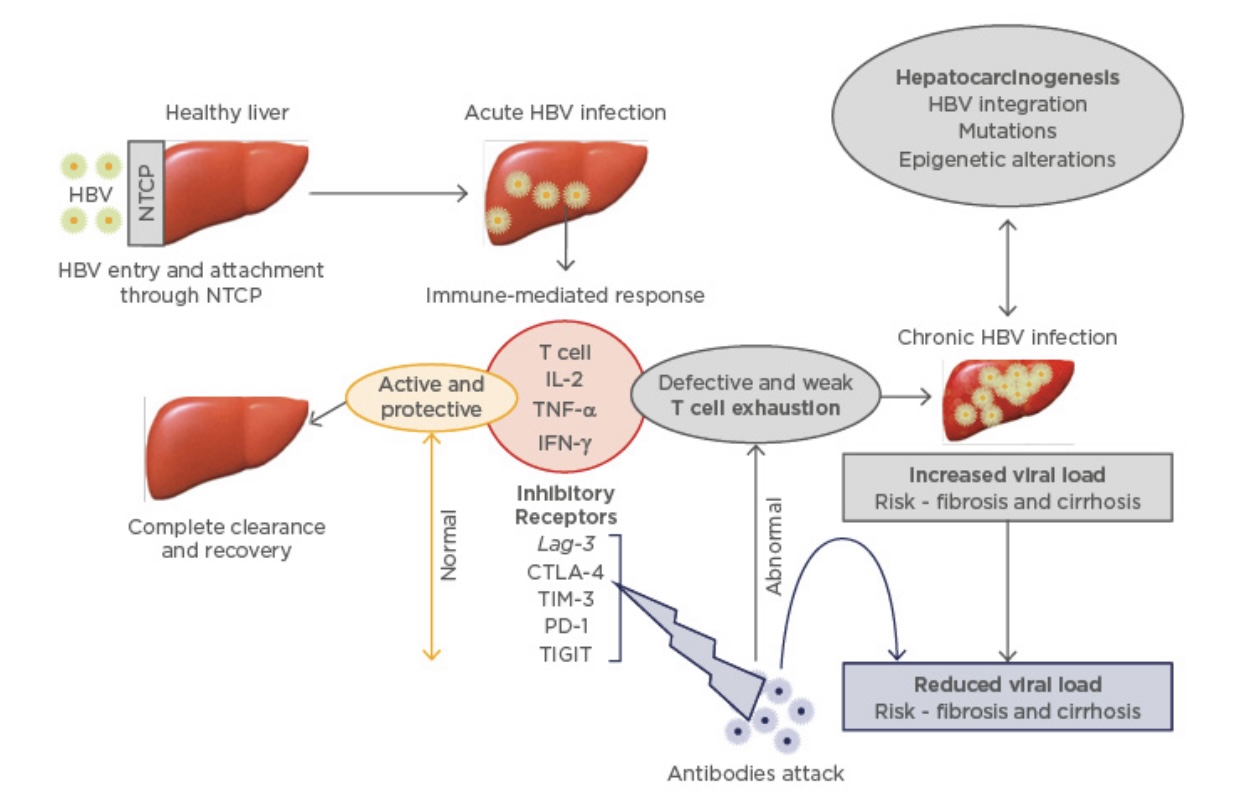
3. What is the pathogenesis of the illness due to Hepatitis B?
Virus enters the liver through blood stream either skin(needle prick) or mucosal contact
“A hallmark in the pathogenesis of HBV infection is its’ variability. Among acutely infected adults, up to 65% develop a subclinical infection characterized only by the appearance of one or more viral antibodies in the blood, while another 25% develop acute resolving infection, which may or may not include a bout of hepatitis. The remaining 10% of patients develop chronic infection (i.e., the persistence of virus and virus antigens in the blood for more than 6 months). In chimpanzees and woodchucks acute infections are characterized by the nearly complete clearance of virus from the blood and liver followed by seroconversion from surface antigen to corresponding antibody. In this case, virus is mostly cleared by non-cytolytic cytokines (e.g., interferon gamma [IFNɣ] and tumor necrosis factor alpha [TNFα]) prior to the appearance of T and other inflammatory cells in the liver, suggesting that most virus clearance occurs prior to the development of acute hepatitis. Further work showed that CD4+ and CD8+ T cells, natural killer (NK) cells, Fas, various IFNs and corresponding receptors, and the TNF receptor 1 participate in virus clearance, suggesting redundant pathways inhibit HBV replication in the liver . The subsequent contribution of a T cell response appears to clear virus infected cells by cytolytic mechanisms involving Fas and granzymes. In this context, CD4+ T cells are required to prime CD8+ T cells to facilitate virus elimination in acute infection . When this happens in acute, resolving infection, the T cell response to HBV is vigorous, polyclonal and multi-specific, while among those who go on to develop chronic infection, adaptive immunity is relatively weak and narrowly focused, suggesting that clearance of HBV is T cell dependent. When T cell responses are not adequate, CLD may develop and progress to cirrhosis and HCC. However, CLD may spontaneously resolve at any of these stages. While the origin of this variability is not completely characterized, it is clear that the ability of the host to mount adaptive immune responses is a key element to limiting virus spread.”
Source: https://www.intechopen.com/books/liver-cancer/pathogenesis-of-hepatitis-b-virus-associated-chronic-liver-disease


4. Is it necessary to have a separate haemodialysis set up for hepatits B patients and why?
Yes it is absolutely necessary to have separate hemodialysis units set up for hepatitis B patients.
chances of HBV transmission through dialysis unit is very high(10% among patients) it is better to have separate units.
5. What are the efficacies of each treatment given to this patient? Describe the efficacies with supportive RCT evidence.
Tenofovir for treatment of HBV
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5220271/
Octreotide for any upper GI bleed
Lasix for fluid overload AKI ON CKD
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4956320/
vitamin k for delayed coagulation
Monocef for AKI (?CKD)
Lactulose for preventing and treating hepatic encephalopathy
https://pubmed.ncbi.nlm.nih.gov/21971378/
6) 58 year old man with Dementia
Case report details: http://
1. What is the problem representation of this patient?
This a case of 58 year old man with complaints of slurring of speech since 6 months,deviation of mouth to right side with drooling of saliva( probably due to bells palsy),since 6 months probably due to bells palsy.
Urinary incontinence and dribbling of urine since 6 months
The patient is forgetting the way to his own house and is wandering,he is forgetting simple things like wearing chappal and is giving delayed response to commands.
He stopped working(he is a saree maker)
Dysphagia to both solids and liquids and a decreased appetite
And this forgetfullness is due to alzeihmers disease
2. How would you evaluate further this patient with Dementia?
Testing types of memory- working memory,episodic memory(anterograde and retrograde),semantic memory,remote memory and implicit memory.
*early alzheimers disease causes loss of anterograde episodic memory(ability to remember an adress after 5 min
Minimental status examination: A thorough cognitive assessment
Which includes the given below picture

3. Do you think his dementia could be explained by chronic infarcts?
Yes, the dementia is due to multiple infarcts in the brain,these are basically silent strokes due to infarcts,these are unindentified and the main cause of dementia like in that of alzheimers
Multi-infarct dementia symptoms can vary, depending on the portions of the brain that are affected. People with this disorder can experience:
- Confusion and agitation
- Problems with memory or difficulty thinking
- Numbness or tingling
- Urinary frequency or incontinence
- Difficulties with attention, concentration and judgment
- Lack of emotion
- Withdrawal from social interaction
- Difficulty planning ahead
- Delusional thinking
- Hallucinations
- Problems with language
- This patient is experiencing some of the symptoms mentioned above
4. What is the likely pathogenesis of this patient's dementia?

Source: https://www.researchgate.net/figure/Pathophysiological-mechanisms-for-vascular-dementia_fig1_311939112
5. Are you aware of pharmacological and non pharmacological interventions to treat such a patient and what are their known efficacies based on RCT evidence?




Comments
Post a Comment